Earlier this year, I purchased Dante Labs “whole genome Z” service, which includes 30x sequencing of every base pair of my DNA, plus an additional 100x on the protein coding regions.
I mostly did this for the raw data. I work in this space and I like to tinker. Using my very own data shields me from any concerns about privacy, consent, and appropriate usage. It’s also super useful professionally: I’m an advisor to folks who are responsible for health and genetic data from hundreds of thousands of patients and research participants. I find that handling my very own information has a way of clarifying my thinking around privacy, consent, and other topics related to good data stewardship.
My experience thus far with personalized genomics is that there’s not a huge amount of diagnostic or clinical value there unless you’re dealing with cancer, the risk of inherited conditions, or a challenging undiagnosed disease. I’m in my 40’s now. I would already be aware if I carried any of the most readily diagnosed genetic disorders.
The joke is that 23andme told me that I’m probably male, most likely of northern European ancestry, sorta average height, probably brown eyes, likely brown hair … you know … all things you could tell at a glance by looking at me.
Aspirin
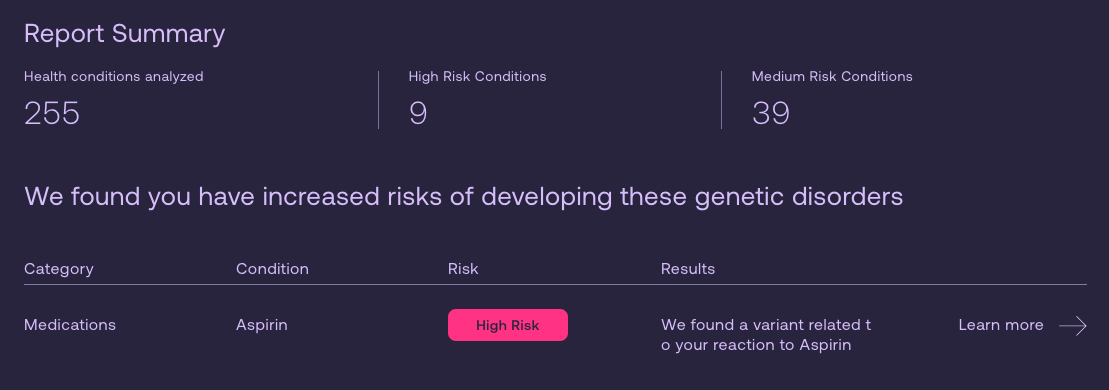
My expectations were low when Dante Labs sent a note inviting me to check out their new “wellness and lifestyle” report. I was 100% surprised to see that the first item on the list was a “high risk” for “Aspirin.” That’s new for me, and I was sort of hoping that the new data had unearthed some heretofore un-observed risk factor.
Spoiler alert: It had not.
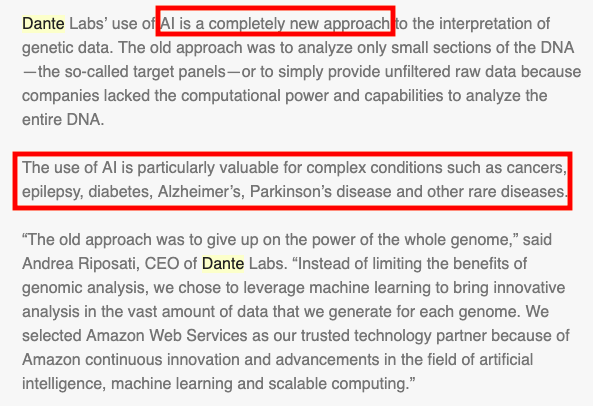
I clicked in to see details, and got this rather opaque wall of generated text, which had obviously never been edited by a human. Maybe that’s what they meant when they claimed to be revolutionary in their use of artificial intelligence in these reports.
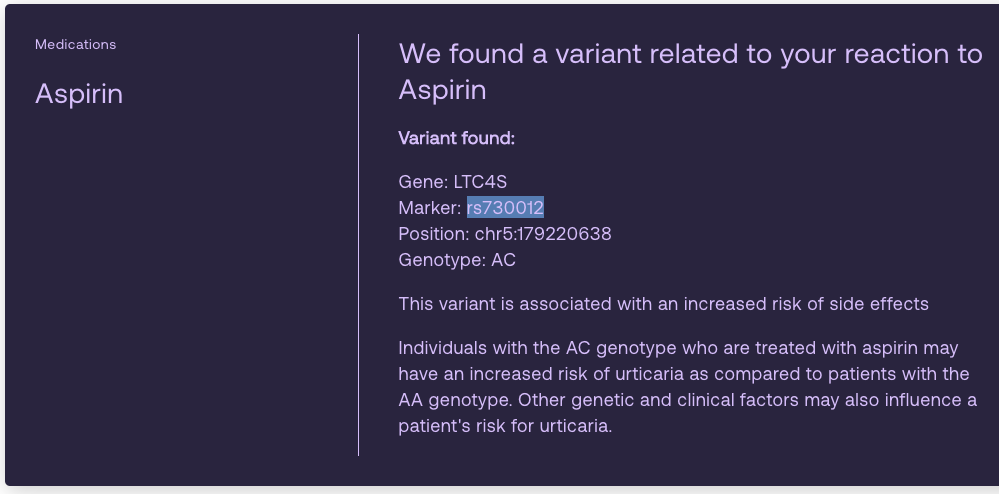
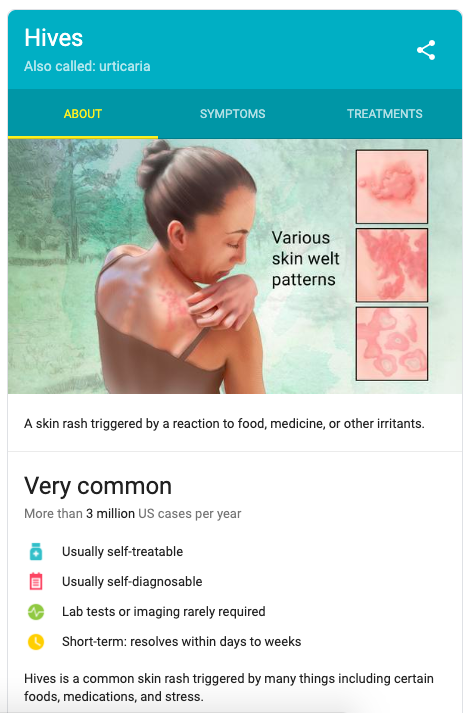
I didn’t know the word “urticaria,” so I googled it. It’s hives: red, raised, bumpy, itchy skin. Millions of people have it, it’s irritating, completely self diagnosable, and eminently self treatable.
I got curious. I take daily low dose aspirin because I’ve read about a constellation of positive effects. The question is, should I stop?
The really simple clarifying question would have been “do you break out in hives when you take aspirin?” The answer to that is “no,” but bear with me, I’m telling a story here.
Nerding out on genetics
The first question with any kind of genetic diagnosis is whether the data is correct. Fortunately, I’ve been a genomics fanboy for a while, and I was able to crack open my raw data from 23andme. Yes indeed, at position 179,220,638 on chromosome 5 I am heterozygous – with an “A” on one of the copies and a “C” on the other.
> grep rs730012 genome_Christopher_Dwan_v1_v2_v3_Full_20170926071925.txt > rs730012 . 5 . 179220638 . AC
After verifying data quality, the next question is “how sure are we about this?” There is a lot of truly tenuous associative research out there, and a naive approach is almost certain to lead you astray.
I took a look at ClinVar, a remarkably powerful and well curated database of the clinically actionable variants. It said that yes indeed, there is an association between this variant and an allergic reaction to aspirin.
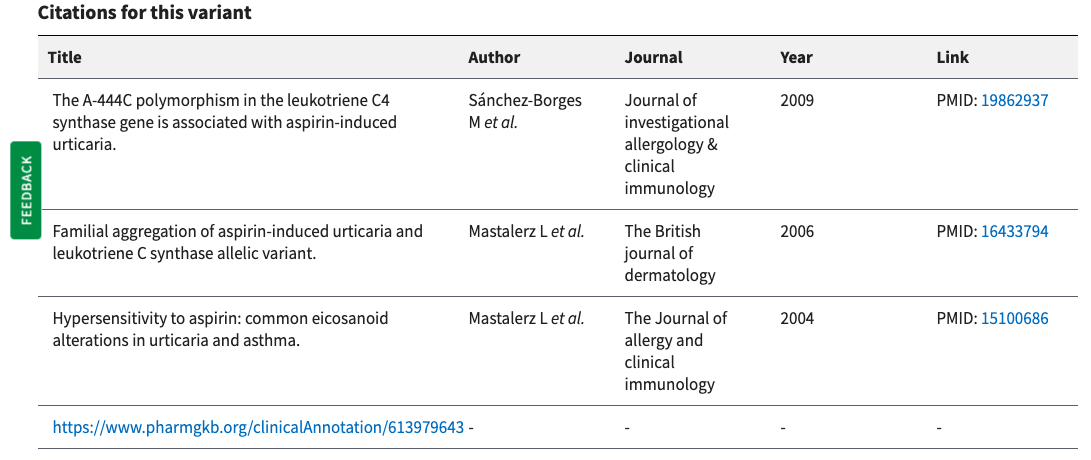
I skimmed the abstracts of the three publications, and while it’s a clear association, it’s not the strongest of signals. The three studies were pretty small, with case and control groups of around 100 people each. Importantly, all three studies asked the question “is this genetic variant more common in people who break out when they take aspirin,” rather than asking the deeper and much more challenging question of -why- such people might have such a reaction.
Short version: It turns out that the reaction to aspirin is more common among people with a “C” at that position at either or both copies of your chromosome 5. In industry parlance, I’ve got one copy of the “risk variant.”
One really important question when looking at this sort of thing is to determine how rare this genetic variant is. My friends at SNPEdia have done a great job of parsing a bunch of different resources to show the answer. In this case, the answer is that among caucasians, my genotype is actually the most common type. It’s pretty rare in other populations, but for white folks like me – most of us have either one or two copies of the risk variant.
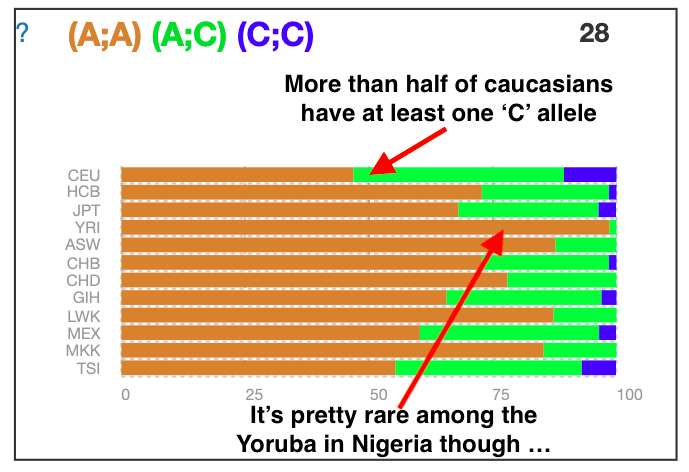
So what you have here is a super common genotype that’s associated with a minor, self diagnosable and self-treatable condition.
So should I stop with my daily aspirin? The answer is probably not.
Other genes, other diseases
SNPedia is my go-to for quick reads on genes and variants. I did a little poking around on aspirin and found a ton of interesting stuff. As just a single example, we’ve got Rs6983267 over on Chromosome 8.
Don’t look at me like that. All interesting people have at least one odd hobby where the nerd-o-meter reads “extreme.” This is one of mine.
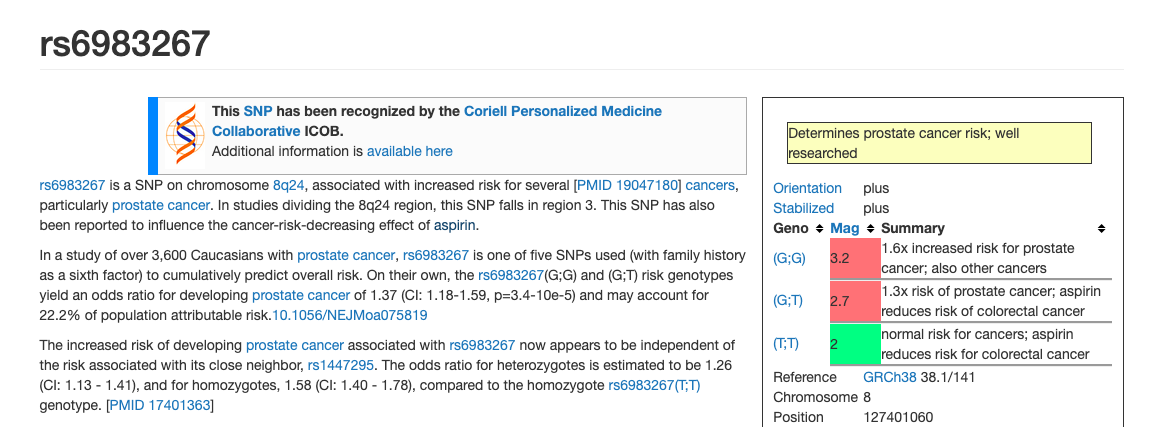
There’s a study of more than 3,000 caucasians with the exact kind of cancer that killed my grandfather, and I have the risk variant (‘GT’) here too. The middle red box on the right, next to ‘GT’ says “aspirin reduces the risk of colorectal cancer.”
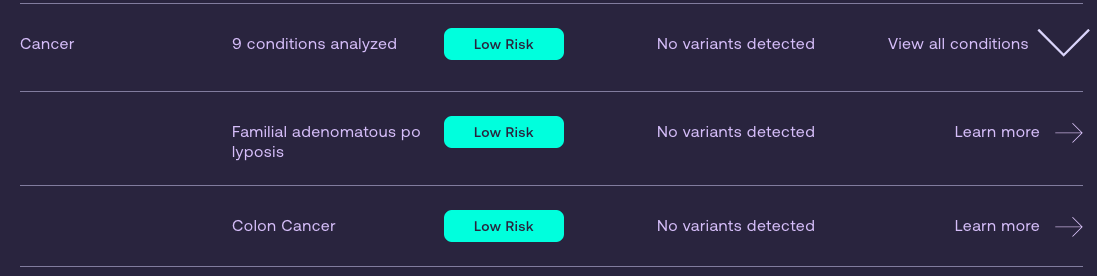
Sadly, this one didn’t make the cut for Dante Labs. According to them, I’m 100% free of colon cancer markers.
So what’s the point?
The point is this: This stuff is complicated and it is important. I’ve written before about how the risk averse culture in American medicine holds us back. This is a counterexample. A naive person might have looked at that report and said “oh hey, I’ll stop taking aspirin, I’ve got a risk factor.” The simple fact is that the risk is for a minor, eminently detectable condition, and there’s good data to suggest that taking aspirin (specifically, for me) reduces my risk of dying painfully of a kind of cancer that runs in my family.
I don’t want the FDA to shut Dante Labs down, but I do want Dante to get their act together and stop just yammering about “AI.”
A side note
In the course of writing and editing this, I have noticed a confounding factor.
Over the past couple of years, I -have- in fact noticed a couple of reddish patches on my torso. I’ve treated them with antifungals, but it didn’t have an effect. They don’t itch and they aren’t terribly visible, so I don’t worry about them.
So, just now, here at the end, I’m thinking that I might cut out the aspirin for a month and see if those patches fade. In that case, I will have learned something. After that, I will 100% resume the aspirin, because duh.
